After the hard work of creating a candidate drug -- the initial insights to try out a particular compound in some chemical search space, the enormous high-throughput screening of small variations on a lead molecule, extensive animal testing -- the promising drug needs to actually be tested in humans. We call these tests clincial trials. There are typically four different types of clinical tirals:
- Phase I: testing the drug in healthy humans to check for toxic side effects and maximum dosage
- Phase II: testing the drug in a few people with the disease group the drug is meant to test to check for efficacy
- Phase III: scaling up to many people in the disease group, check for side effects
- Phase IV: studies after initial approval, typically on a patient group already tested in a previous phase and run for a longer time period
Running trials is hard work; you've got to screen for patients, track patient progress, measure many things, keep results organized for months or years.
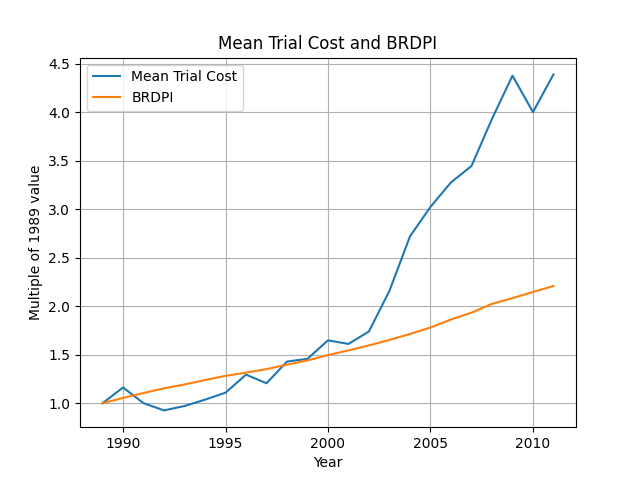
A 2014 study by Berndt and Cockburn found that costs for trials were increasing really quickly. (This study, and a lot of others I've found, is based on Medidata's PICAS database -- I wonder if I can get access to that?)
(There are other trends that contribute: namely number of patients and the geographic distribution is changing with Phase I/II recruiting less and Phase III/IV recruiting more, but that shouldn't show up much when discussing cost per patient.)
Really quickly compared to what?
The NIH publishes the Biomedical Research and Development Price Index (BRDPI), which indicates how much the NIH budget must change to maintain purchasing power. That's a good starting point for checking whether increases in clincial trial pricing are surprising:
How much of this is because of increased site work?
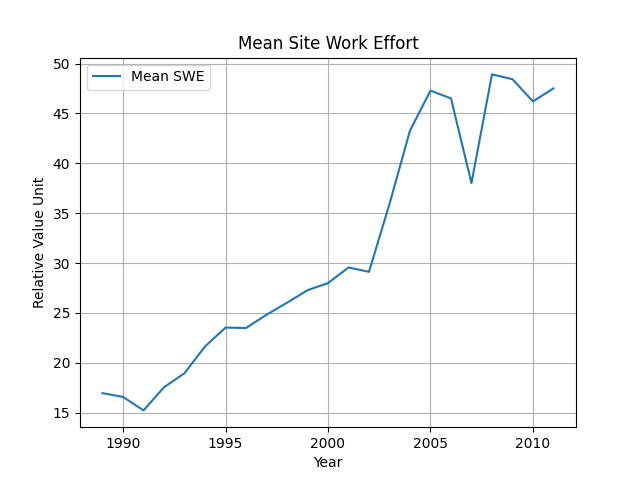
If price is increasing, it might be because trials are contributing more value than they were in the past, eg checking more endpoints, doing more complex procedures. Berndt14 uses a measure of "Site Work Effort" to approximate this:
That seems to follow the rise in prices reasonably well. When we divide the mean price by mean site work effort, we follow the R&D price index more closely:
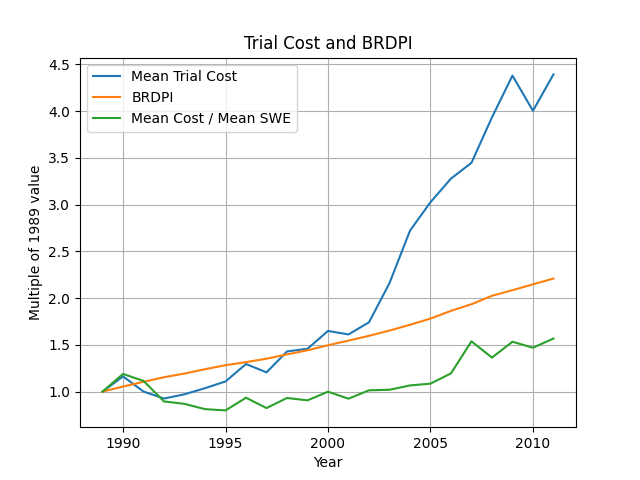
(Well, take this with a grain of salt because \(avg(\frac{a}{b}) \neq \frac{avg(a)}{avg(b)}\).)
What is site work, concretely?
Work is measured in relative value units (RVU), which are a Medicare measure of value added by a physician service. If some services provided during clinical trials don't have a Medicare RVU, the authors rely on a panel of physicians at Tufts to estimate the time spent per procedure.
Here are some common types of procedures with their occurences per trial protocol from Getz08:
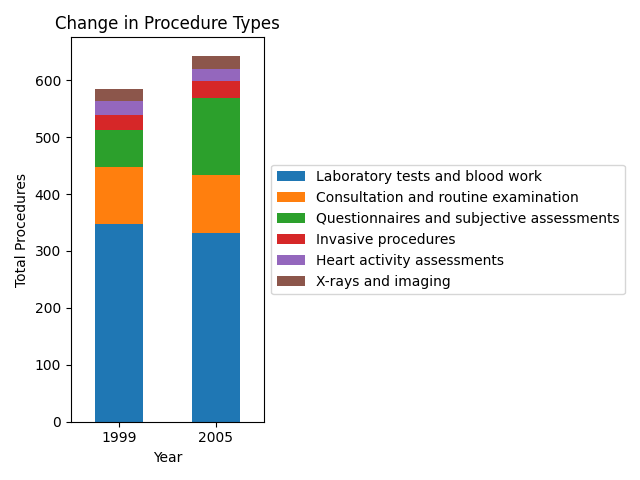
It'd be useful to check how this varies with therapeutic class. Getting into the details of which procedures are common for different therapeutic areas and which sorts of procedures require the least amount of effort or are the most scalable seems important. I shied away from doing this analysis because having just two data points (1999, 2005) really means the analysis isn't very helpful. I'll look for more recent studies before continuing the analysis.
Can we tease out any trends about economies of scale?
Berndt14 does some regression analyses to look for relationships between cost-per-patient and total number of patients in a trial or total site work effort.
Here I've plotted the regression coefficients for how cost-per-patient (TGPP: total grant cost per patient) depends on total number of patients. This is a log-log regression: \(\ln(\text{TGPP}) = b + a \ln(\text{NPATIENTS})\), where \(a\) is the regression coefficient being graphed. Notice that for "economies of scale", we'd want the regression coefficient to be negative: average cost decreases as number of patients increases.
(Aside: we're doing a log-log analysis to focus more on elasticity. If we used just \(\text{NPATIENTS}\) and \(\text{TGPP}\), the analysis would tell us that a one-unit increase in former causes an \(a\)-unit increase in latter. If we use the logarithms of both, the analysis instead tells us that a 1 percent increase in former causes an \(a\) percent increase in the latter.)
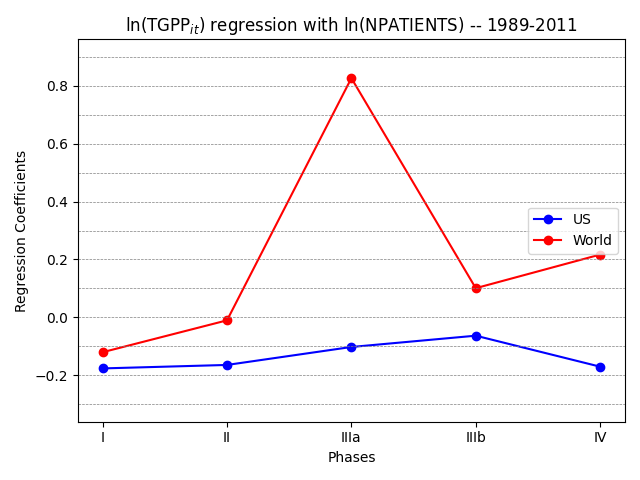
This is alarming! Trials in the US have slight economies of scale, but trials in the rest of the world have huge diseconomies of scale in Phase III and IV. Economies of scale are really only relevant in Phase III and IV trials because they have hundreds or thousands of patients, while earlier phases have tens of patients.
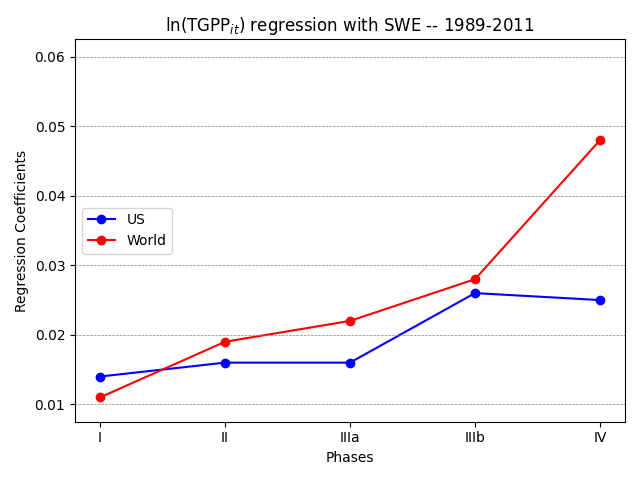
Here's another regression analysis for how log cost-per-patient varies with site work effort. We expepct this to be positive: more work probably means each patient is more expensive. (Here we're looking at a semi-log analysis: a one-unit increase in SWE causes an \(a\) percent increase in TGPP.)
Why does the rest of the world have large diseconomies of scale?
I'm still working on this, and I'll spin it out into a separate post! Do email me if you have any ideas for how to investigate this.